
Hospital Billing Is a Crime Against American Patients

PARIS – Last month, I experienced some symptoms that mimicked a possible heart attack. It turned out to be a false alarm, and I’m fine. But taking no chances, we headed for the emergency department at the American Hospital of Paris, where I’ve been living this fall. I got a complete workup: a full physical, cardiogram, blood tests, a scan to check for possible clots, and a consultation with doctors. The care was efficient and superb. It all took less than four hours.
At the end of the visit, when I was pronounced in good health, I was presented with the bill: 875.57 euros, or about $890 at prevailing exchange rates. At a good hospital in the U.S., the bill would have been at least $10,000, maybe double that, mostly paid by insurance.
The visit to the ER alone, before a single test was done or care was provided, would have been billed at more than the total cost of my workup in France. In the U.S., the average ER “facility” charge is $1,201.
My visit was such a bargain compared with standard billing practice at U.S. hospitals that I wondered if I was somehow being subsidized by the French medical system. So I sought out one of France’s leading experts on hospital financing and comparative hospital systems, Dr. Isabelle Durand-Zaleski, who is both a professor at the University of Paris and a practicing physician.
Dr. Durand-Zaleski reviewed my bill, which was conveniently displayed in a single page with clear line items. She confirmed that these were the hospital’s actual costs, and the identical bill would have been sent to the French social security system, had I been a French citizen. And, bien sûr, the French citizen would have paid nothing out of pocket.
HOW ARE AMERICAN HOSPITALS able to bill at 10 or 20 times these rates? And how does their billing strategy interact with the near-collapse of the American hospital system?
There are several parts to the answer. One is that there is no direct price regulation in the U.S., so hospitals are free to charge what they think the market will bear.
The market in this case is mostly insurance companies. Hospitals have been on an orgy of mergers and acquisitions to increase market concentration and bargaining power relative to insurance companies. In Boston, where mergers have reduced hospitals to two large systems, the big hospitals tell the insurers, if you want your subscribers to be able to use Mass General, or Beth Israel, you have to pay our charges.
This is partly in reaction to health insurance industry consolidation across America. Concentration on one side of the transaction begets concentration on the other side. My colleague David Dayen has called this “concentration creep.”
Most hospitals in the U.S. are either for-profits, or nominal nonprofits like large teaching hospitals that behave just like for-profits. Their goal is to maximize market share, particularly for the most lucrative specialized procedures. That means they spend a great deal of capital, not just on acquisitions but on construction of new facilities (that may be redundant in many cities) and on new costly equipment.
As we’ve seen, a French hospital bills actual costs. By contrast, an American hospital adds to the bill several layers of overhead, each with exorbitant markups. The capital cost of a merger is part of your bill, along with the capital cost of the equipment.
For instance, in the U.S. when you get a scan, you are being billed for part of the capital cost of the scanner, plus the hospital’s markup. In France, you pay a flat rate that has been negotiated with French social security, based on how long you were in the room, any materials such as injectable dyes, and the salary of the technician. My scan was billed at 280 euros. In the U.S., the average price of an inpatient CT scan is $4,750.
My Brandeis colleague, professor Stuart Altman, a national expert on hospital costs who was the longtime chair of the Massachusetts Health Policy Commission, the state agency tasked with restraining costs, calculates that at more than $6,000 per patient, U.S. hospitals have triple the capital costs of Europe’s hospitals. Meanwhile, every major European nation not only spends far less on health care but has much better outcomes in terms of every major health indicator.
The more complex the billing strategy is, the more it adds to costs. Expenses related to billing add about $99,000 per year per clinician, or about one-seventh of a hospital’s costs, according to a study in the Journal of the American Medical Association. Another study, published in Health Affairs in 2014, found that administrative costs accounted for 25.3 percent of all hospital costs in the U.S. health system. If anything, that number is higher today.
In principle, Medicare could use its extensive bargaining power to cut hospital charges. But Medicare is very timid about challenging hospital billing practices and is reluctant even to crack down on the notorious abuse of “upcoding”—assigning the most expensive reimbursement code possible to every patient condition. If I once had, say, benign heart palpitations, and I go to the hospital for knee surgery, the hospital would assign a code allowing it to bill at a higher rate on the premise that I’m also a heart patient.
Medicare could save taxpayers a lot of money. Why are they so timid? Because hospitals in many areas are the largest and most politically powerful local employers, even more so when they are teaching hospitals connected to universities. Don Berwick, who headed the Centers for Medicare & Medicaid Services (CMS) under President Obama, told me, “If CMS ever tried to seriously crack down, their phone would ring, from the American Hospital Association, local senators and congressmen, and the White House.”
ONE OF THE MANY REGULATORY FAILURES of antitrust in the U.S. is the nearly complete failure to challenge hospital mergers and acquisitions, which have created monopoly power and degraded services in city after city. When the FTC has tried to move, it has been overruled by conservative courts.
Even worse, many of these merger binges are by hospital systems that are nominal nonprofits, such as Mass General Brigham in Boston and the University of Pittsburgh Medical Center. In New York, Mt. Sinai is now an eight-hospital system. In Philadelphia, the courts overruled an effort by the Federal Trade Commission to block a merger by two nominally nonprofit systems, Thomas Jefferson University and Albert Einstein Healthcare Network, which together now control 18 hospitals and at least 60 percent of inpatient services. According to a study published in Health Affairs, seven of the ten most profitable hospitals in United States are technically not-for-profits.
Hospitals also overuse specialists, who can bill at higher rates. Back in the day, if you had, say, a small wart, your family doctor would remove it. Today, you are likely to be referred to the dermatologist for anything more complex than a hangnail, and of course the dermatologist can bill at a much higher rate, some of which is shared with the hospital as profit.
But here’s the irony. This general business strategy is backfiring, not only on patients but on hospitals. Most large hospitals today are losing money. They have overspent on capital equipment and lavish facilities and acquisition of doctors’ practices to attract patients for the most lucratively reimbursable procedures. That adds costs and leaves less money for basic care.
Boston is now suffering from an emergency room catastrophe. This is no longer about COVID; there are few such cases in ERs. The Boston Globe recently reported standard eight-hour waits in the emergency room at Mass General. People were piled up on gurneys in hallways.
“It’s unprecedented in my career,” Dr. Michael VanRooyen, chief of emergency medicine at Mass General Brigham, told the Globe, adding that about 6 percent of people who sought treatment in the ER gave up and went home without being seen.
The ER pileup is substantially the result of staff shortages. RNs have burned out from the hellish working conditions, and many have left the profession. This is another vicious downward spiral. If there were more adequate staffing levels and better pay, there would be less nurse burnout. But hospitals spend so much on acquisitions and facilities for the most lucrative procedures that they can’t find enough money for basic clinical staffing. And because of the political power of hospitals, nurse staffing ratios are one more fundamental that is unregulated or unenforced in most states.
When Mass General, Boston’s oldest and most distinguished hospital, entered into a joint operating agreement with the Brigham and Women’s Hospital in 1994, the new parent corporation was named Partners HealthCare. It later occurred to the corporate leadership that this bland branding was squandering one of Boston’s most familiar and prestigious brands, the Mass General Hospital. Brigham was also right up there.
So, in the contest for market share, the execs at Partners decided in 2019 to take their branding full circle. They spent a cool $100 million on a campaign to re-rebrand Partners as … wait for it … Mass General Brigham. Sheer genius. Imagine if some of that had been spent on nurses, or emergency rooms.
Executive pay is also exorbitant. Anne Klibanski, chief executive of Mass General Brigham, earned $4.3 million in total compensation in 2020, the most recent year for which IRS tax forms are available. Her predecessor, David Torchiana, took home $6,128,085 in 2019. Nine executives received more than a million dollars.
Despite its nonprofit status, which generates massive tax breaks, Mass General Brigham does not deign to publish annual reports disclosing either salary information or details of its relative outlays and capital investments. It does disclose its quarterly profit or loss. You could actually get a lot more information from mandatory SEC filings if it were a for-profit—which it is in everything but name and legal form.
THERE WAS A TIME, before the allure of market competition and profit-maximizing took over, when hospitals were more heavily regulated. Two basic mechanisms that prevented the game of padding bills were direct rate regulation and certificates of need.
Until the 1980s, in most states hospital rates were directly regulated, a system known as all-payer rate setting. They still are in Maryland, whose costs are far below average. But rate regulation was phased out in most places in favor of market competition.
In that era, most states and the federal government also required “certificates of need” before hospitals could buy expensive new equipment that might duplicate equipment available elsewhere in the service area. In the era of deregulation, certificate-of-need regulation was also scrapped or weakened, leaving hospitals free to purchase often redundant capital equipment that adds to the rate base. In fact, certificates of need have now become a barrier to entry for startup hospitals, which must navigate the regulatory thicket to get cleared to buy equipment, while dominant rivals who have mastered the system skate by.
A variety of market-friendly techniques were devised to contain costs. Hospitals proved expert at gaming all of them.
The most highly touted was called DRGs, or diagnosis-related groups. The idea was that the insurer would pay the hospital a flat sum, based on the average cost of treating a given condition, rather than paying by the day or by the suture. This way, the hospital would be incentivized to use the most efficient treatment modalities rather than the most lucrative. Dream on.
The concept was first devised by researchers at Yale in the early 1970s. New Jersey was the first state to implement a version of it. And in the 1983 budget legislation, DRGs were mandated for Medicare.
How did that reform work out? In 1983, health care accounted for just under 10 percent of GDP in the U.S. Today, it is almost 20 percent.
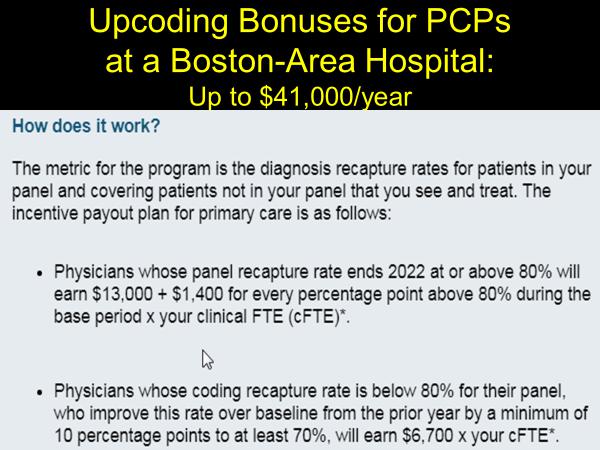
The hospitals’ response to DRGs was more corrupt upcoding. One Boston-area hospital offers physicians incentive payments of up to $41,000 per year for upcoding. Here is a handy chart based on materials sent by the hospital to doctors explaining how the incentives work (thanks to Drs. David Himmelstein and Steffie Woolhandler).
Until recently, advocates of single-payer health care have focused on comprehensive coverage but less so on the abuses of profit-maximizing medicine. If we went to Medicare for All but did not reform these billing practices and did not end the system of profit-maximizing medicine entirely, these excess costs would simply be piled onto taxpayers.
Rep. Pramila Jayapal’s current Medicare for All bill does best at addressing these abuses, and Bernie Sanders’s latest version is more attuned to them than his earlier bills.
Under Jayapal’s bill, co-sponsored by about half of the House Democratic caucus, the system would keep some elements of fee-for-service medicine and diagnosis-related coding, but hospitals would operate under “global” budgets. That is, they would receive an annual flat sum from the government that would be adjusted regularly to reflect caseloads. Medical education—one of the ways that teaching hospitals pad bills—would be its own separate budget item. Capital outlays and staffing ratios would be regulated. Incentive compensation aimed at gaming the system would be prohibited. There would be much greater emphasis on primary care.
This legislation, which merely reflects common practices in most European nations, is at the outer fringe of what is even debated in the U.S. It is a reminder of how inefficient as well as unjust is market-led medicine, and how incremental reforms can never repair our broken health system.
Robert Kuttner is co-founder and co-editor of The American Prospect, and professor at Brandeis University’s Heller School. His latest book is Going Big: FDR’s Legacy, Biden’s New Deal, and the Struggle to Save Democracy.
Read the original article at Prospect.org.
Used with the permission. © The American Prospect, Prospect.org, 2022. All rights reserved.
Click here to support the Prospect's brand of independent impact journalism.