
Sunday Science: Polio Is on the Brink of Eradication. Here’s How To Keep It From Coming Back

Nobody expected polio to be back.
It’s 2040, a decade since the disease was eradicated. The global health campaign that vanquished the virus has disbanded; immunization efforts have slackened. Then, one day, a sick child in a conflict-wracked country develops paralysis; the cause turns out to be polio. Scientists trace the origin of the virus to a laboratory on the other side of the world. A technician at the lab had handled a forgotten batch of polio-infected material — and then visited their family abroad.
As cases multiply, the World Health Organization (WHO) appeals for help to conduct emergency immunization campaigns, but stocks of vaccines are low and few members of staff have direct experience of polio outbreaks. Soon there are tens of thousands of cases: millions more people around the world who haven’t had the vaccine are at risk.
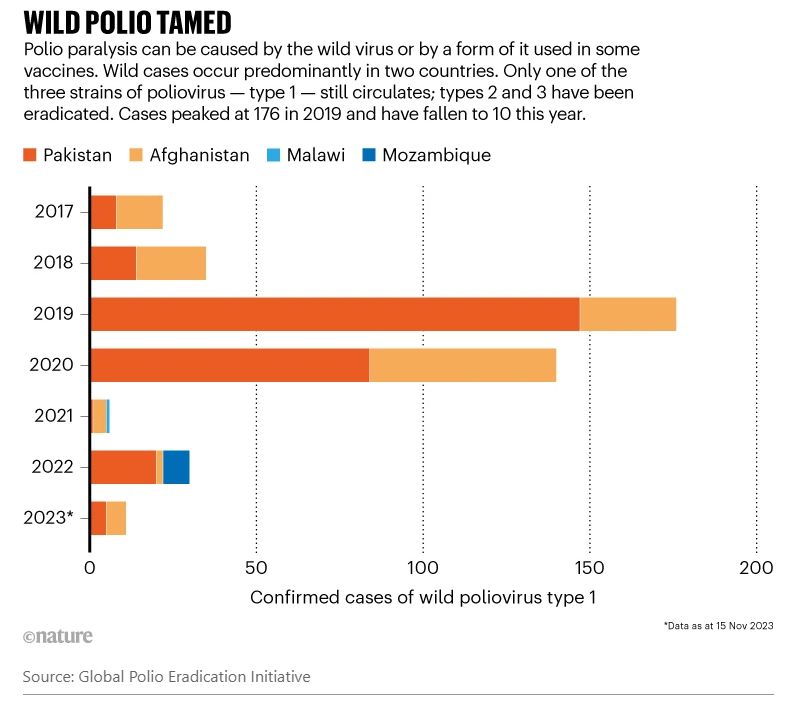
This is just one of many possible scenarios that could follow polio eradication. Although the world has not yet eliminated poliovirus, many observers think it could be gone within three years. The polio-eradication campaign has increased its intensity and funding in the past year in the hope of finally meeting a deadline that’s been postponed many times since efforts were launched in 1988.
The front lines are Afghanistan and Pakistan, where pockets of wild polio persist but are shrinking (see ‘Wild polio tamed’), and a swathe of Africa, where a polio vaccine that includes live virus has itself seeded outbreaks. There are signs that health campaigns are now bringing these vaccine-derived episodes under control.
The final steps towards eradication are formidable, and it’s not clear when — or whether — nations will reach this goal. Nonetheless, with the demise of the virus in sight, health authorities are planning what happens next.
That’s because eradication is not extinction. Polio could lurk in testing labs and manufacturing facilities — from which it has leaked in the past — and even in some people. Mistakes years after eradication could let polio into an unprotected population where it could “wreak havoc”, says virologist Konstantin Chumakov, former associate director of vaccine research at the FDA Office of Vaccines Research and Review in Silver Spring, Maryland.
The end of polio is only the beginning of another effort: developing the resilience to keep it away, says Liam Donaldson, a public-health specialist at the London School of Hygiene & Tropical Medicine, UK, and the lead author of a series of independent reports on the campaign’s progress (see go.nature.com/49hho4a). “People have signed up to polio eradication, but they’ve not signed up to the longer journey.”
Stamping it out
Only one human disease has so far been declared eradicated: smallpox, in 1980. Polio has been more complex, says David Heymann, who heads the WHO’s Containment Advisory Group. That’s because of a key difference: every smallpox infection produces symptoms, but polio can silently infect up to 1,000 people before causing a case of paralysis. The other snag is that polio can be caused not only by the wild virus, but also, in very rare cases, by the vaccines deployed to prevent it. Eradication means getting rid of both forms for good.
The main tool is vaccination. Industrialized, polio-free countries use an inactivated poliovirus vaccine (IPV), which doesn’t prevent the virus infecting the body and being shed in stools, but does protect against paralysis. Provided that immunization levels with IPV remain high and sanitation is good, a rogue poliovirus will probably peter out, according to Concepcion Estivariz, a polio researcher at the Centers for Disease Control and Prevention (CDC) in Atlanta, Georgia.
But because the inactivated vaccine can’t block transmission, children in at-risk countries still receive another type: an oral poliovirus vaccine (OPV) that contains an attenuated form of the live virus, and can stop polio’s spread — which is crucial for eradication. It’s also cheaper and easier to deliver than IPV, which is administered by injection. The oral campaign has been hugely successful. Since 1988, the Global Polio Eradication Initiative (GPEI) estimates it has prevented 20 million cases of polio paralysis.

A chemist processes samples at the National Polio and Measles Laboratory in Bangladesh. Credit: G.M.B. Akash/Panos
But OPV has some important downsides. There is a low risk that the vaccine itself can cause paralysis. And, on rare occasions, the weakened virus used in the vaccine can mutate sufficiently to regain virulence. This can lead to outbreaks of cases known as vaccine-derived polio among people who have not been vaccinated fully or at all. “If we continue OPV,” says Estivariz, “we never stop the circle.” Most countries are now using IPV in their routine immunization programmes alongside OPV, and the WHO recommends that IPV administration should continue for a decade after disease transmission has been stopped, to protect against any accidental releases or hidden pockets of the virus.
Polio will be certified as eradicated when no case has been observed for three years, and when there is no sign of it in environmental surveillance data — that is, in samples of waste water. A year after that, OPV must be withdrawn to prevent vaccine-derived polio. The problem, however, is that removing it will be an extraordinarily delicate manoeuvre. Done messily, this process could trigger the return of the virus.
In 2016, for instance, the withdrawal of an OPV across 150 countries went disastrously wrong. “The results were sobering”, says Kimberly Thompson, an epidemiologist at the research non-profit organization Kid Risk, in Orlando, Florida.
There are three strains of wild polio — types 1, 2 and 3. Type 2 was declared eradicated in 2015, and type 3 followed in 2019. The oral vaccine contained attenuated versions of all three strains, but after type 2 was eradicated, the aim was to withdraw vaccines containing that strain to minimize the risk of seeding vaccine-derived type 2 polio. So the GPEI orchestrated a two-week period in April 2016 in which all three-strain oral vaccines were switched for versions containing just types 1 and 3.
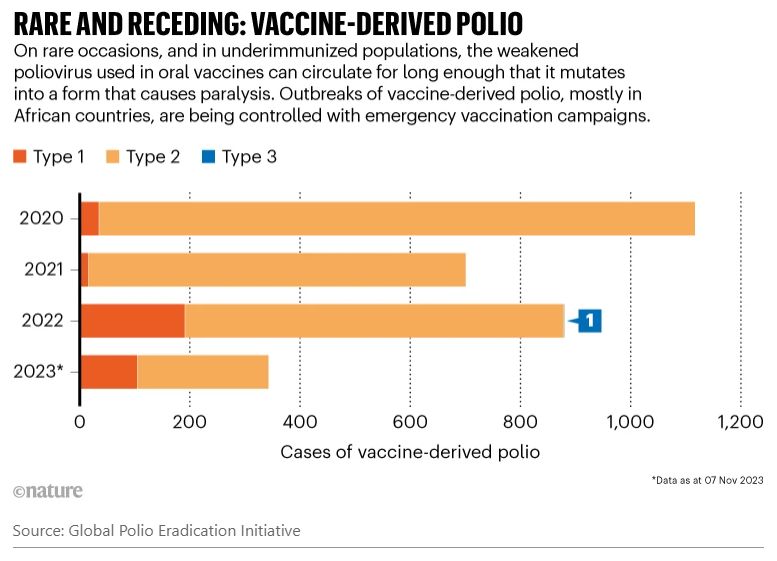
Swiftly, however, cases of vaccine-derived type 2 polio began to build — in two countries in 2016, spreading to 24 countries by 2020, with countries in Africa worst affected. A case popped up in the United States in 2022, and the United Kingdom found the virus in wastewater samples. The cumulative number of paralysis cases so far is just over 3,200; the yearly total peaked at more than 1,000 in 2020 and now seems to be declining, with 238 recorded so far this year (see ‘Rare and receding: vaccine-derived polio’). African countries are still running multiple emergency campaigns delivering oral type 2 vaccines to stamp these outbreaks out.
Why the rebound? First, populations in the regions affected weren’t sufficiently vaccinated beforehand with IPV, which would have protected them until any outbreaks could be controlled. This was partly owing to a gap in vaccine supply, says Ondrej Mach, who co-chairs a new GPEI group that will oversee future withdrawals of the oral vaccine.
What’s more, says Mach, just before the switch, vaccine-derived type 2 polio was detected in Nigeria. Transmission was probably already under way in Nigeria and other countries, adds Mach, and the emergency type 2 vaccine seeded further outbreaks.
Since 2021, however, this seeding has become much less likely: vaccination campaigns are controlling the outbreaks using a genetically engineered oral vaccine, which has an even lower chance of becoming virulent than the OPVs used previously.
What risks does the post-polio world face if full oral withdrawal goes wrong? An analysis by Kid Risk and the CDC gave one answer (D. A. Kalkowska et al. Risk Anal. https://doi.org/k428; 2023). Their model considers what might happen if all OPV use stopped in 2027 but vaccine-derived polio was not completely eliminated beforehand and outbreak responses were weak. In one scenario, the model predicts that there could be as many as 40,000 cases of paralysis caused by vaccine-derived polio 8 years after OPV administration is discontinued. To avoid this, the authors suggest that population immunity in areas with polio cases today needs to be very high — about 90% — just before withdrawal. Thompson says that most countries have achieved this in the past, at least for short periods of time.
Keeping a lookout
Even after OPVs are successfully withdrawn, therefore, countries can’t let their guard down. They must put in place surveillance “to detect any poliovirus, no matter where in the world it appears and however fleetingly”, says a report by the Transition Independent Monitoring Board, an independent group of scientists that reports periodically on the polio endgame and is chaired by Donaldson.
Polio surveillance takes two main forms: searching for cases of paralysis that might be caused by polio; and monitoring waste water for any virus shed by carriers.
Both will be crucial for years, as an example from Malawi shows. The country had been free from wild polio for three decades when, in 2021, a stool sample from a three-year-old with paralysis arrived at the national laboratory to be sent abroad for testing. The sample sat for two months before it was shipped with others, says Jamal Ahmed, who coordinates polio eradication for the WHO in its African region, which comprises 47 countries. The result came back a month later: it was wild polio type 1, not seen in the continent since 2016.
Sequencing traced its origin to Pakistan, but also revealed that the virus had been circulating for two years undetected — possibly in Malawi, and possibly elsewhere. Because Malawi had no wastewater surveillance at the time, it was impossible to know.

A health worker gives an oral polio vaccine to a child in Karachi, Pakistan, in 2022.Credit: Asif Hassan/AFP via Getty
Within 30 days of receiving the result, emergency immunizations began. Six campaign rounds later, says Ahmed, Malawi has seen no more cases of wild polio. And, with the WHO’s help, the country swiftly installed environmental surveillance sites.
The episode also showed that the emergency vaccination programme wasn’t up to the job, says Jay Wenger, who leads the polio programme at the Bill & Melinda Gates Foundation in Seattle, Washington. “We had to rebuild the polio infrastructure we had before” to get rid of the virus, he says.
Global wastewater surveillance has become a bigger priority since the COVID-19 pandemic, says Donaldson, because politicians are paying more attention to trends in disease. Ahmed says that 41 of the 47 member states of WHO Africa now have environmental polio surveillance, and that the rest will soon catch up.
Innovations are helping to speed up a process in which timeliness is crucial. One breakthrough is direct detection, a method that leapfrogs several of the conventional stages of the testing process; for example, by extracting RNA directly from samples without the need to culture them.
The threat of escape
No matter how successful the eradication effort is, the virus will remain in research institutes and vaccine-manufacturing facilities — and in an unknown number of routine diagnostic labs.
Escapes happen. Last year, a lab worker at a manufacturing facility in Utrecht, the Netherlands, picked up type 3 virus at the facility, and this was then detected in wastewater surveillance outside the plant. No cases of paralysis resulted. Vaccine manufacturing is “a huge containment nightmare”, says Mach.
The WHO has a plan for poliovirus containment that urges nations to minimize the number of facilities retaining poliovirus materials and to destroy any unnecessary stocks. At the moment, the WHO knows of 74 facilities that hold polio, in 22 countries.
The first step was for each country to set up a national authority for containment by 2018, to ensure that facilities comply with biosafety requirements. China and Romania have not yet done this, and other countries have missed subsequent deadlines.
Even for compliant facilities, forgotten samples remain a threat, says Andy Macadam at the National Institute for Biological Standards and Control in Potters Bar, UK. “All you have to do is mislabel the tube.” And polio might lurk in some facilities that are not even subject to the containment plan, says Heymann. This could include frozen stool samples taken for other reasons at a time when polio was circulating.
Since 2000, there have been 21 reported incidents of poliovirus release from laboratories and vaccine-production facilities in 8 countries, with 16 cases of polio as a result, according to Derek Ehrhardt, who heads the WHO’s poliovirus containment unit. Most cases have been in vaccine-manufacturing facilities, but five of them were in research labs in which workers discovered that vials containing poliovirus were mislabelled (none of those cross-contamination incidents led to paralysis). The solution, says Heymann, is better biosecurity in all labs.
To reduce the need for live virus, scientists are developing ways to produce the inactivated vaccine without it — for example, by using a non-infectious, genetically engineered starting material, or by designing vaccines from virus-like particles or messenger RNA.
A surprising source
There is yet another source of poliovirus, unforeseen 35 years ago when eradication efforts began.
In most people who receive the oral vaccine, the immune system generates antibodies that protect them against the virus. But in a small number of people born with particular immune deficiency disorders, the immune system allows the attenuated virus from the vaccine to live on, evolving as time goes by and emerging in their stools. No drugs have been proved to cure an ongoing polio infection.
Only some of the several hundred types of immunodeficiency lead to chronic retention of poliovirus. No one knows how many people are affected, and no such shedding is known to have triggered a polio outbreak, although it might have contributed to one in the Philippines in 2019–21.
But, says Mach, even one person retaining and shedding poliovirus is incompatible with eradication. “We have to do something.” An international — if patchy — search for people with these immune disorders who have chronic polio has produced a register of 200 individuals.
One person with the condition lives in the United Kingdom and was vaccinated with OPV as a child. For more than 20 years, he asymptomatically carried — and shed — the attenuated virus, which evolved to its disease-causing form. His gut was “essentially a culture vessel”, says David Boyle at PATH, a non-profit medical-research organization based in Seattle, Washington.
That’s why scientists were surprised to learn that the person’s infection had gone.
It disappeared after he received the antiviral drug remdesivir for severe COVID-19 in August 2021. This could be coincidence, says Macadam, but it bolsters the case that antivirals could be used to treat polio infection (two such drugs are being explored as polio treatments). Monoclonal antibodies are also under development.
Complacency and responsibility
Keeping vaccination rates high for at least a decade after eradication will be the best protection — but there are fears that commitment to IPVs might wane once eradication has been declared. Routine immunization campaigns struggle to reach every child, especially during conflict, disasters or pandemics. COVID-19 drove the number of unvaccinated or undervaccinated children up to 23 million in 2020.
Added to this is the growing problem in some regions of vaccine scepticism and complacency, which grew worse because of activism against COVID-19 vaccines, says Peter Hotez, a vaccine specialist and public advocate at Baylor College of Medicine in Houston, Texas.
With so much to be done to maintain a polio-free world, Donaldson is asking who will be accountable once the GPEI disbands a year after eradication, handing its responsibilities to WHO departments, partners and national health programmes.
A transition has already begun in some countries, but many have struggled to find their own funding amid changing government priorities. Slackening efforts now could bring bigger problems in the future, says Aidan O’Leary, who directs polio eradication at the WHO. “If we collectively take our eye off the ball and don’t build the resilience of health systems going forward, then we face further problems down the line.”
But done well, says O’Leary, the post-polio world could bring wider health benefits for everyone: better surveillance and immunization measures, and more joined-up health services. “The last mile of the polio eradication programme”, he says, “is the first mile for global public-health security.”
Nature 623, 680-682 (2023)
doi: https://doi.org/10.1038/d41586-023-03602-5
Aisling Irwin is a freelance journalist writing mostly about science, the environment and development whose work regularly appears in New Scientist, Nature, SciDev.
Nature is a weekly international journal publishing the finest peer-reviewed research in all fields of science and technology on the basis of its originality, importance, interdisciplinary interest, timeliness, accessibility, elegance and surprising conclusions. Nature also provides rapid, authoritative, insightful and arresting news and interpretation of topical and coming trends affecting science, scientists and the wider public.
Nature's mission statement
First, to serve scientists through prompt publication of significant advances in any branch of science, and to provide a forum for the reporting and discussion of news and issues concerning science. Second, to ensure that the results of science are rapidly disseminated to the public throughout the world, in a fashion that conveys their significance for knowledge, culture and daily life.
Nature's original mission statement was published for the first time on 11 November 1869.
Study: The Indo-European language family was born south of the Caucasus
By Frank Jacobs
Though over three billion people speak an Indo-European language, researchers are not sure where the language family originated.
Strange Maps
September 16, 2023