
Curing Cancer: Conquering Disease or Creating Profit?
MIA In The War On Cancer: Where Are The Low-Cost Treatments?
Jake Bernstein
ProPublica
April 23, 2014
http://www.propublica.org/article/where-are-the-low-cost-cancer-treatments
This story was co-published with The Daily Beast
Michael Retsky awoke from surgery to bad news. The tumor in his colon had spread to four of his lymph nodes and penetrated the bowel wall. When Retsky showed the pathology report to William Hrushesky, his treating oncologist, the doctor exclaimed, "Mamma mia."
"Michael had a mean looking cancer," Hrushesky remembers.
Retsky didn't need anyone to tell him his prognosis. Although trained as a physicist, he had switched careers to cancer research in the early 1980s and spent more than a decade modeling the growth of breast cancer tumors. During his treatment, he joined the staff of one of the most prestigious cancer research labs in the country.
In the absence of chemotherapy, there was an 80 percent chance of relapse. Even with therapy, there was a 50 percent chance the cancer would return. The standard treatment was brutal. Six months of the highest dose of chemotherapy his body could withstand and, after that, nothing but hope.
Like many cancer patients, Retsky didn't much like the odds. Unlike most cancer patients, however, he had the knowledge to question them. His own research had sown doubts that standard chemotherapy, as used the world over to treat colon and some breast cancers, was always the best approach. In collaboration with Hrushesky, the two devised an inexpensive, low-impact chemo treatment following surgery that dripped smaller doses of the drug into his body over a longer period of time.
Seventeen years later and cancer free, Retsky cannot be entirely sure the treatment cured him, but he believes it likely did. Numerous laboratory, animal and small human studies suggest that low-dose, continuous chemotherapy holds promise in shrinking tumors and preventing cancer's recurrence. But the next step — testing what Retsky did in a large-scale clinical trial — is a longshot given the way cancer treatments are developed today.
Take Michelle Holmes, an associate professor of medicine at Harvard Medical School. She's been trying for years to raise money for trials on the effects of aspirin on breast cancer. Animal studies, in vitro experiments and analysis of patient outcomes suggest that aspirin might help inhibit breast cancer from spreading. Yet even her peers on scientific advisory boards appear uninterested, she says.
"For some reason a drug that could be patented would get a randomized trial, but aspirin, which has amazing properties, goes unexplored because it's 99 cents at CVS," says Holmes.
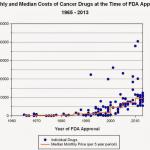
Increasingly, Big Pharma is betting on new blockbuster cancer drugs that cost billions to develop and can be sold for thousands of dollars a dose. In 2010, each of the top 10 cancer drugs topped more than $1 billion in sales, according to Campbell Alliance, a health-care consulting firm. A decade earlier, only two of them did. Left behind are low-cost alternatives — therapies like Retsky's or existing off-label medications, including generics — that have shown some merit but don't have enough profit potential for drug companies to invest in researching them.
The newer drugs have in some cases shown dramatic life-extending results for patients. Yet cancer remains the second-most-common cause of death in the U.S. after heart disease, killing about 580,000 people a year. Worldwide, 60 percent of all cancer deaths occur in developing countries, where experts say the incidence of the disease is growing rapidly, as is a desperate need for affordable care. That has added urgency to an active debate about whether efforts to combat cancer — and where to put scarce research dollars — need to be rethought.
"If we are winning the war on cancer, we are not winning that fast," says Vikas Sukhatme, Harvard faculty dean for academic programs at Beth Israel Deaconess Medical Center in Boston and the Victor J. Aresty Professor of Medicine at Harvard Medical School.
Sukhatme and his wife Vidula, an epidemiologist, are among those trying to do something about it. They have spearheaded a new nonprofit, Global Cures, to promote alternative treatments that are unlikely to attract commercial interest from drug companies.
Global Cures calls these forsaken therapies, " financial orphans." To help patients and their doctors, the nonprofit is producing reports that explain the science behind promising orphan therapies — those that have shown merit in animal studies and limited human data. And Global Cures also has set itself a more challenging goal — to find the money for clinical trials.
In one example, Retsky and a team of collaborators are exploring whether an inexpensive dose of a generic painkiller before breast cancer surgery might reduce lethal recurrences of the disease. If results in a small retrospective study of 327 mastectomy patients in Europe were to bear out, the anti-inflammatory drug ketorolac could save thousands of lives a year in the United States alone, Sukhatme has estimated.
The data behind the treatment are only suggestive, however, and more testing is required. Retsky and his colleagues have been unable to raise the millions of dollars a large-scale trial would need to make a real determination, in part because no drug company has the incentive to fund such a study, they say.
Without the confirmation of large-scale human trials, doctors are reluctant to approve patient use of orphan therapies, even in cases where there is little else to offer. It's a challenging conversation when a patient suggests an alternative medication to a doctor, who despite having the ability to prescribe off-label, doesn't want to risk making the situation worse. "It borders on crossing the line between good evidence-based medicine and simply trying to deal with the desperate hopes of desperate patients," says Allen Lichter, chief executive officer of the American Society of Clinical Oncology. Nonetheless, Lichter acknowledges that there are financial orphans that do not get the review they deserve.
The financial orphan problem points to a deeper issue with the way cancer drugs are developed. Pharmaceutical companies exist to make a profit and cannot be expected to cover many important areas of research that go unexplored, according toLarry Norton,deputy physician-in-chief for Breast Cancer Programs at New York's Memorial Sloan Kettering Cancer Center.It's a gap in the system.
"The biggest challenge we have today is not necessarily the science," Norton says, "it's creating a business model that makes sense."
In 1993, about a year before Retsky received his colon cancer diagnosis, he attended a breast cancer conference in Europe. An Italian scientist named Romano Demicheli presented data from a decades-long study of breast cancer patients. Demicheli also had been a physicist but had switched to oncology research after his wife died of Hodgkin lymphoma in 1976. Like Retsky, Demicheli doubted the dominant view of how cancerous tumors grow.
In a landmark study from the 1960s, Anna Laird at the Argonne National Laboratory had published research showing that tumor growth was predictable. They started fast, grew at an almost exponential rate and then slowed, she wrote. More than 500 scientific papers cited Laird. Based in part on these studies, chemotherapy was developed to attack tumors aggressively in the early, high-growth stage when they presumably would be most vulnerable.
Retsky's research into the data had convinced him there was nothing linear about tumor growth. Instead, he found that they developed erratically and sometimes experienced periods of dormancy before reawakening. Demicheli's presentation offered another insight into the progression of tumors.
Data from the Istituto Nazionale dei Tumori in Milan, where Demicheli is a senior researcher, showed two distinct patterns of relapses in a sample of 1,173 Italian women who had undergone breast cancer surgery but no additional treatment. One grouping of relapses came around 18 months after surgery, and a second smaller one cropped up around 60 months.
At the same conference, Retsky saw a presentation by Michael Baum, a professor of surgery at the University College London who later became president of the British Oncological Association. Baum, looking at British databases, had come to a similar conclusion: There were two distinct waves of post-surgical breast cancer recurrence.
Over the next few years, the men met and began to kick around the obvious questions: What was causing that first wave of recurrence? And what did it mean for cancer treatment?
A third question hovered unspoken over the conversation: Who would pay to find out?
Creating an innovative new drug — including everything from early research to late stage trials — costs on average of $1.3 billion, according to the Tufts Center for the Study of Drug Development. The Food and Drug Administration has taken steps to speed up the process for approving cancer drugs. Nonetheless, drug development in the United States, even when it is funded in part by taxpayer dollars and encouraged by federal bureaucracies, isn't geared toward inexpensive alternative treatments.
Five Low-Cost Drugs That Might Combat Cancer
These five medications were approved for other uses but also have shown potential cancer-fighting properties that the nonprofit Global Cures says merit clinical trials.

The bulk of funding the U.S. government dedicates to research on diseases like cancer goes to basic science and is funneled through the National Institutes of Health (NIH). It is research that might not be done but for taxpayer investment. Federal dollars helped produce such scientific breakthroughs as the human genome project.
The NIH, particularly through the National Cancer Institute, contributes to about 15 percent of all clinical trials related to cancer, but the amount it gives is in decline. In 2012, the NCI spent about $754 million on clinical trials, or nearly $100 million less than in 2008. To leverage the money, the NCI seldom funds an entire trial by itself. The agency instead partners with pharmaceutical companies or academic institutions, and the trials the NCI does support usually are for new drugs, not for repurposing existing ones. Of the 1,785 trials the agency is backing at the moment, only 134 are for the larger and costlier late-stage human trials known as phase III.
The NIH recognizes that commercial drug development has its limitations. For example, a new NIH program targets what researchers call the "Valley of Death." This area encompasses the research that comes before key human studies, where treatments often languish for lack of funding or attention. One NIH pilot project encourages drug companies to let researchers study compounds that are under patent but are no longer being explored. In 2013, the NIH gave $12.7 million spread over nine projects. The effort does not focus on inexpensive alternatives that could be made available quickly, according to John McKew, acting scientific director for preclinical innovation at the NIH's National Center for Advancing Translational Sciences.
Holmes, the Harvard professor, says money sets the agenda for cancer drug development. "What is scientific and sexy is driven by what can be monetized," she says, "and that becomes the norm."
In September 2013, the British Health Service launched a randomized aspirin trial, something Holmes has been struggling to do in the United States. The trial, which will run through 2025 and involve thousands of patients, looks at whether aspirin taken after standard curative treatments can improve survival and reduce the recurrence of breast, colorectal, prostate and gastro-esophageal cancers.
A summary of the trial explains that concerns about toxicity, particularly the risk of bleeding, are among the reasons aspirin hasn't been studied for primary prevention of cancer.For patientswho have already been treated, however, the potential benefitas a follow-up therapymay outweighthe risks. If aspirin is shown to work, "it could be implemented in both resource rich and resource poor countries and would have a huge impact, improving cancer outcomes worldwide," the summary says.
Low-cost alternatives like aspirin must fight for consideration within a scientific community that is producing effective cancer drugs that can command $100,000 or more for a course of treatment. The escalating prices for these drugs worry many involved in the fight against cancer. Some of the new drugs will eventually be used in combination, a step that could push cost of treatment into the hundreds of thousands, says Lichter.
"There is a point at which the equation breaks down and you can't support the whole treatment process anymore," he says. "We need to have an environment where we can have new drugs at a price that allows us to use those drugs and still allows these companies that have invested in them to reap a profit. But how we get from here to there is not clear."
The Pharmaceutical Research and Manufacturers of America, the major trade group representing the world's top drug companies, declined to comment about financial orphans. A spokeswoman for the group provided a white paper that makes the case that there has been "substantial progress in the fight against cancer." The impact of new drugs takes years to fully realize, and therapies being developed for single indications may eventually be useful for other cancers, the paper says.
"It is important to keep in mind that innovative medicines are what provide the next generation of generic medicines," Sally Beatty, a spokeswoman for the drug company Pfizer, says in an emailed statement from the company.
The predominant focus of cancer drug development today is on "targeted therapies" that are both innovative and lucrative. These drugs block the growth and spread of cancer by interfering with specific molecules involved in tumor growth. Fashioning these targeted therapies involves costly molecular and genetic experimentation, but once patented the investment can translate into enormous drug company profits.
Total number of world cancer cases, 2012
57%
of all cancers are in developing countries
Source: World Health Organization
The Swiss multinational company Novartis created one of the first targeted drugs. Gleevec treats myeloid leukemia and has turned a terminal disease into a chronic one for many patients. In 2012, Novartis had $4.7 billion in global sales from Gleevec. Last year the FDA approved its use for another kind of leukemia that affects children. Novartis declined a request to comment on the issue of financial orphans.
A subset of targeted therapies involves shutting down the ability of cancer cells to evade the body's immune response. Immunotherapy, as the treatments are called, was long seen as a failed approach until recent molecular breakthroughs. Now, the promise of immunotherapy is ratcheting up the stock prices of several companies that are developing drugs along these lines.
One of the first to get a drug in this class to market was Bristol-Meyers Squibb, with Yervoy. Even though the drug is only approved for advanced melanoma, an aggressive skin cancer, it grossed $960 million last year. A course of treatment goes for about $120,000. Bristol-Meyers also declined a request to comment on the issue of financial orphans.
Some of the financial orphans Global Cures identifies are believed to enhance the immune response to tumors. Without more study it is difficult to isolate exactly why they operate the way they do. Vidula Sukhatme says this is one of the chief complaints she and her husband receive from scientists who disagree with their approach. "They call them 'dirty medicine,'" she says. "They say, 'The whole world is going toward targeted therapies and you are going backwards.'"
Sukhatme believes that what matters more than an understanding of the precise mechanism is whether a drug works. It's possible that these alternatives may have synergistic effects that cannot be reduced to a single molecular target, she says.
Even before his cancer diagnosis, Retsky had dug out the original Laird papers from the medical library at Penrose Hospital in Colorado Springs, where he was a professor at the University of Colorado. The initial study was based on observations of tumors in only 18 rodents and one rabbit. Earlier studies contradicted the findings.
After Retsky weighed the evidence, he decided not to risk his recovery on standard chemotherapy. In January 1995, after surgery to remove his tumor, Retsky was ready for treatment. Yet he was no doctor. An oncologist would need to supervise.
Retsky found Hrushesky, a cancer doctor who split his practice between the Department of Veterans Affairs Albany Stratton Medical Center in New York and another local hospital. Hrushesky had worked with the National Cancer Institute doing therapy evaluation and had gained attention for a theory that the ill effects of chemotherapy could be minimized based on the time of day it was administered. To accommodate patients getting chemotherapy at odd hours, Hrushesky used a pump that operated automatically. He also gave low doses of chemo to patients with late-stage cancers whose bodies couldn't withstand conventional high-dose therapy. Six years later, the approach would be dubbed "metronomic therapy" by another researcher.
As he sat in Hrushesky's waiting room, Retsky wondered how the oncologist would greet his unconventional proposal. Hrushesky came out in cowboy boots and proceeded to shake the hand of every patient in the room. Retsky liked him immediately.
In the therapy, Retsky received low doses of a standard chemotherapy agent called Fluorouracil (5-FU) through a pump while he slept at night. The hole in his chest through which the drug flowed required some fussing, but there was no discomfort. The therapy lasted two and a half years, a period Retsky chose based on his estimates of tumor growth and the amount of chemo needed. In aggregate, Retsky received a larger dose of 5-FU than the standard concentrated therapy. Other than a few blood blisters in his mouth and slight skin cracking on his hands, Retsky experienced none of the worst chemo side effects, like nausea, fatigue and hair loss, he and Hrushesky say.
During his therapy, Retsky took a job with the research team of Dr. Judah Folkman, a renowned cancer researcher whose Boston laboratory ushered in new understandings of the way tumors grow. Retsky says he and Folkman, who has since died, went to a meeting with a top scientist at the Dana Farber Cancer Center in Boston, one of the foremost cancer treatment centers in the country, to pitch an exploration of metronomic therapy.
No one was interested. Retsky says they were told it was most likely the surgery rather than the follow-up treatment had stopped his cancer. It's not an unreasonable response, he says. Without more research, there is no way to know for sure.
Metronomic therapy is a quintessential financial orphan, Vikas Sukhatme says. It has some promising data behind it, but why it appears to function is not well understood. Retsky used a relatively cheap generic. Independent researchers in Canada, Europe and India are exploring similar inexpensive agents with metronomic therapy. The low cost provides little incentive to pharmaceutical companies to investigate but makes it a source of great interest to the developing world.
In 2000, Folkman's researchers published an animal study of metronomic therapy and found that it seemed to limit tumor growth. Around the same time, a cancer researcher in the department of medical biophysics at the University of Toronto, Robert Kerbel, did an animal study that reached similar conclusions. Randomized human studies involving hundreds of European and Japanese patients who underwent a metronomic therapy have shown improved survival rates.
The approach still faces hurdles beyond just the uncertainty about how it works. One theory, Kerbel says, is that metronomic therapy triggers an immune response in addition to chemo's traditional toxic effect on cancer cells. But pinpointing a proper dose is challenging, as are the ethics of involving patients with early stage cancers, he says. A trial could needlessly endanger patients either by exposing them to a toxic drug they didn't need or causing them to forgo a better-established treatment.
Nonetheless, a French pediatric oncologist, Nicolas André, is trying to promote metronomic therapy in the developing world and has organized a foundation to pay for studies. "Will we ever be able to treat cancer for US$1 a day?" he asks in a recent paper. "The answer might be an absolute yes, provided we encourage scientific research and clinical studies on metronomic treatments."
Retsky is less confident that metronomic therapy using 5-FU on early stage colon cancer will ever receive trials in the United States. "The drug was less expensive than sterile water," he says, "so no pharmaceutical company would spend millions of dollars testing it if there was no financial reward."
The data that led Retsky and his colleagues to recognize the two waves of relapses and the erratic growth of tumors also carried them into the fiercest dispute over breast cancer of the past 20 years: When should women have mammograms?
One of his collaborators, Baum, had helped establish the mammography program for England's National Health Service in the 1980s. The thinking behind it was self-evident. Catch the tumor early. Save a life. But the reasoning only made sense if the tumor grew in a linear, predictable way.
It was also possible, Baum theorized, that the tumors might never progress; they might remain dormant for long periods of time or, less likely, could even shrink. By the 1990s, studies had begun to suggest that mammograms, for younger women, were not helpful and possibly were harmful. Women in their 40s who received mammograms had a slightly higher mortality rate than women who did not. Called the "mammography paradox," the phenomenon remains controversial. Baum concluded money would be better spent on treatment rather than mammography.
The toolkit for treating aggressive breast cancer once it migrates to another part of the body remains limited. The majority of the approximately 40,000 U.S. women who die from breast cancer annually do so when the cancer reappears in another part of the body after surgery. There is no cure once the disease has gone metastatic, according to a report by the Department of Defense Breast Cancer Research Program. The median survival term for metastatic breast cancer is about three years, a number that hasn't statistically changed in two decades.
In 1997, Retsky and Demicheli published a paper suggesting that it might be the breast cancer surgery itself that was causing the first wave of relapses they had identified. A computer simulation based on the data of Italian women Demicheli had studied suggested that removal of a primary breast tumor from premenopausal women with cancer in a lymph node triggered a cancer growth elsewhere in about 20 percent of cases. A few years later, Baum posited that the math behind tumor growth looked more like chaos theory than anything else. He, too, suggested that surgery might play a role in breast cancer recurrences. The trio, as well as Folkman and other researchers in their group, published several more papers along the same lines, but it wasn't until 2005 that their theories entered the mainstream.
"We weren't running to newspapers and issuing press releases," says Retsky. "We were just looking at the data and presenting it to our colleagues in the scientific community."
In 2005, Retsky, Demicheli and Hrushesky published a report in the International Journal of Surgery that offered surgery as a theory to explain both the mammography paradox and the first relapse wave. The paper did not propose that women forgo surgery — only that the data suggested a need for more research. But this time, an article about their report in The Wall Street Journal brought the idea to the wider public, where it was pilloried as dangerous because it might scare women from a vital treatment option.
What exactly connected surgery and the cancer recurrence remained a mystery to Retsky and his collaborators, who proposed and discarded various hypotheses. By this time, Retsky was a lecturer at Boston's Children's Hospital and Harvard Medical School and the author of multiple scientific papers. He was asked to review a case study out of Lebanon that had cited his work. It described a patient with advanced cancer who had bumped his head. Tumors had grown at the site of the bruise. Retsky couldn't explain why, but a colleague at the Folkman lab suggested he look at inflammation. Animal studies showed a correlation between inflammation and cancer growth. And surgery also caused inflammation.
From there grew the idea that inflammation itself could be a facilitator of metastatic growth. Retsky and his colleagues theorized that the act of creating wounds in surgery spurred the body to growth as part of the healing process. This in turn might spread the cancer cells. If this was true, intervention to save breast cancer patients had to begin prior to surgery, the researchers concluded.
In 2010, Retsky and his collaborators came upon a paper published in the journal of the International Anesthesia Research Society by a Belgium-based anesthesiologist named Patrice Forget. He had looked at retrospective data from a Belgian surgeon whose breast cancer patients had received nonsteroidal anti-inflammatory drugs (NSAIDs) prior to surgery in the hope that they would lessen post-operative pain. Among the NSAIDs used was ketorolac.
After surgery, the patients all received the standard therapy of chemo, radiotherapy and endocrine therapy. The study size was small — 327 patients who had undergone mastectomies between February 2003 and September 2008. Of those 175 had received ketorolac.
Forget found that cancer recurred in 17 percent of patients who did not receive ketorolac and only 6 percent of those who did. The association was statistically significant and held up even when adjusted for age and other characteristics. There was no effect for the other NSAIDs although that may have been a function of not enough patients trying them, says Forget.
Clinical evidence from studies in animals and retrospectively in humans already existed suggesting that NSAIDs might help limit tumor growth. At least one other large retrospective study published in the peer-reviewed journal Cancer Causes & Control reported that NSAIDs might limit breast cancer recurrences. Forget didn't know why ketorolac might work better than other NSAIDs, although he postulated various theories.
Ketorolac, a generic, is considered a relatively nontoxic drug. No single company owns it. The drug can cost as little as $5 a dose and might only be needed once before breast surgery. Retsky says a large-scale clinical trial in India could provide a better patient population for study and be done for as little as a few million dollars. But because it's so cheap, ketorolac offers little in the way of profit incentive.
Retsky met with Brandy Heckman-Stoddard, program director for the Breast and Gynecologic Cancer Research Group for the National Cancer Institute. She had seen one of his presentations at a scientific conference and had been intrigued. "Retsky's work is very provocative, but it is difficult to believe that such a short course of NSAIDs during surgery could have such a dramatic effect on recurrence," she says.
Sloan-Kettering's Norton is also aware of Forget's paper on ketorolac, but he cautions that there are too many potential variables to draw definitive conclusions from a single retrospective study. Although it would not be his first choice for investigation, Norton believes the effects of ketorolac and other NSAIDs on breast cancer are worth exploring and are the types of research for which there is no business model. "Is it a meritorious hypothesis to test?" he says. "Yes, I think it is."
Giving patients ketorolac before surgery is not without risk. In some cases it can lead to bleeding. It's a legitimate issue, says Vikas Sukhatme, and one that surgeons would have to understand. Forget notes that an American Society of Anesthesiologists report approves of ketorolac use for pain prior to surgery.
The National Cancer Institute estimates the current annual cost of breast cancer treatment in the United States at approximately $19 billion. If a single injection of a low-cost drug could save lives and put a dent in those costs, Vikas Sukhatme contends it's worth investing in definitive research about its effectiveness and safety.
"Personally, should I have to choose an analgesic drug [to take before] breast cancer surgery, I would choose ketorolac," Demicheli says. "But it is still a reasonable choice, not a scientifically based choice. To solve the question, at least one high-quality randomized clinical trial is needed."
Widespread acceptance won't come without trials that give doctors confidence. Gauri Bhide, a community oncologist in the Boston area who has consulted with Global Cures and believes in its mission, says she would not prescribe ketorolac. "The surgeons would kill me," she says. "Until someone tells them it is safe to take right before surgery, they are not going to do it."
Forget is trying. After multiple rejections, he cobbled together enough money for a limited double-blind trial that began last year. One of the donors is a small Belgian-based foundation called The Anticancer Fund. Like Global Cures, the group has a dual mission of providing information on alternative cures and encouraging their study. It was started by a wealthy European real estate mogul, Luc Verelst, born from his experience trying to help his sister, who was suffering from uterine cancer.
Still, Forget's study is not large enough to be dispositive. "It's a pilot study," says Retsky. "It's not designed to confirm or deny [if the drug works]."
Money for trials won't come easy. Retsky and his collaborators received a $600,000 multiyear research grant in 2009 from the Susan G. Komen breast cancer foundation. The group turned them down for money for a clinical trial of ketorolac a few years later. Only about 3 percent of Komen's clinical trial investments go to large, final-phase studies, according to a foundation spokeswoman. Retsky's group made it past the first round for funding from the Department of Defense, which has poured almost $3 billion into breast cancer research since 1992. Then money for the DOD program was sidelined by the sequestration budget cuts mandated by Congress, Retsky was told.
One of the drugs Global Cures highlights has found backing for a large-scale trial — though it took Pamela Goodwin, a Canadian oncologist, more than a dozen years of grant writing, meetings and clinical breakthroughs from other researchers to cobble together what will eventually be close to a $30 million study.
The widely used Type 2 diabetes drug metformin, a generic that has been associated with reduced breast cancer risk, is now the subject of a 3,500-patient trial involving 300 medical centers that Goodwin characterizes as bare-bones. The NCI is providing about half the funding, primarily for the U.S.-based centers, with contributions also coming from Canadian nonprofits and the British and Swiss governments.
Given recent cutbacks in U.S. government funding, both Goodwin and Dr. Lois Shepherd, senior investigator with the National Cancer Institute of Canada Clinical Trials Group, believe that what they've done probably can't be replicated.
"If this trial had come forward for approval today, I'm not sure it would be approved — and it has nothing to do with the science," says Shepherd.
The Sukhatmes hope that Global Cures can serve as a matchmaker between researchers who want to conduct trials on promising alternatives and family foundations or other donors that might fund them. The group also plans to use crowdsourcing to raise money from patients and others who may want to donate to trials.
Total number of world cancer deaths, 2012
65%
of all deaths are in developing countries
Source: World Health Organization
Patient groups have become much more active in the way they approach the funding of trials, says Kenneth Kaitin, director of the Tufts Center for the Study of Drug Development, who believes that the research gap identified by Global Cures exists across multiple diseases.
" have a vested interest in seeing the product developed," he says. "Their goal is not to make a lot of money but to get [the drugs] out."
The Sukhatmes hope to create a way for patients to document online the treatments they undergo. Harnessing the experience of cancer patients is also a goal of the American Society of Clinical Oncology, says Lichter, the group's CEO. The society wants to compile and analyze patient experiences nationwide to give better guidance to patients and doctors. "There is a lot of knowledge out there, but it is locked up in individual files and records," Lichter says.
Vikas Sukhatme says Retsky's experience with his own cancer exemplifies what Global Cures hopes to do. Retsky was a patient who, after careful research, adopted a financial orphan treatment and documented the result. The toxicity of the treatment was not bad. Retsky went into it with eyes open and understood the tradeoffs. Although his case is far from conclusive, if there were 50 people like Retsky whose collective data showed strong results, it would build a foundation for further study, Sukhatme believes.
Although Retsky and his collaborators are frustrated about the lack of progress on ketorolac, they are optimistic that scientific advances under way, including the new targeted therapies, will eventually have a real impact. Still, they worry that these new therapies will only be available for the wealthy.
"It is so expensive it makes me weep," says Baum, the British oncologist. "I weep for all the poor people in the world who will never have access to such treatment."
Washington Post Can't Even Talk About Alternatives to Patent Support for Prescription Drug Research
Dean Baker
CEPR
04 May 2014
http://www.cepr.net/index.php/blogs/beat-the-press/washington-post-cant-even-talk-about-alternatives-to-patent-support-for-prescription-drug-research
Just as the media in the Soviet Union were not allowed to talk about alternatives to one-party rule, the Washington Post apparently can't raise the issue of alternatives to patent supported drug research in the United States. This should be apparent to readers of an article on Sovaldi, a new drug to treat Hepatitis C.
The drug is currently subject to a government granted patent monopoly which allows its manufacturer, Gilead Science, to sell a year's dosage for $100,000. By contrast, a generic version sells in India for about 1 percent of this price. As the piece tells readers:
"If all 3 million people estimated to be infected with the virus in the United States were treated with the drugs, at an average cost of $100,000 per person, the amount spent for all prescription drugs in the country would double, from about $300 billion in a year to more than $600 billion."
To put this number in context, the additional cost of Sovaldi due to the government granted patent protection would in this case be equal to more than 1.7 percent of GDP, or a bit less than 25 percent of after-tax corporate profits. In short, it is real money.
One might think that an article that raises ethical questions, as this one does, about how much we should be willing to pay for saving a person's life, might also ask the question about why this drug is so expensive in the first place. Not in the Washington Post.
The granting of patent monopolies is a government policy to provide incentive for innovation. There are other ways to provide incentives, like paying people directly. (Has anyone heard of the National Institutes of Health? They get $30 billion a year to do basic biomedical research.) The government also finances a large amount of research directly through the Defense Department, with military contractors paid to develop new weapons systems. So there is a great deal of precedent for the government paying directly for research.
Some economists, like Joe Stiglitz, a winner of a Nobel prize, have suggested a prize fund where the government would buy up patents and then place them in the public domain. Under either system, all new drugs could be sold as generics at generic prices.
This would meet the condition that the price would then equal the marginal cost, which is usually a high priority for economists. Economists and people who have been through intro econ classes usually get upset when government policies like tariffs raise the price of a product by 15-20 percent above marginal cost. In this case, the patent monopoly is raising the price by close to 10,000 percent above marginal cost.
All the economic distortions and incentives for corruption that we would see from a 15-20 percent tariff also appear when a patent monopoly raises the price by 10,000 percent, except they are several orders of magnitude greater. The company has enormous incentive to mislead patients and doctors about the effectiveness and safety of their drug and also to market for uses for which it may be inappropriate. Drug companies also have incentives to pay off politicians to get their drugs covered by public programs. And drug companies act all the time in exactly the way predicted by economic theory. (Think of Vioxx.)
It is incredible that alternatives to patent supported research were never mentioned in an article that poses ostensibly difficult ethical questions about how much a life is worth.Without the government granted patent monopoly such questions would not arise, unless the Post puts the value of human life at less than $1,000.
It is also amazing that, at a time where much of the intellectual class has been obsessed with Thomas Piketty's book, Capital for the 21st Century, which warns of a growing concentration of wealth and income, a policy that both creates enormous economic distortions and leads to upward redistribution of income, is not even a topic for debate.
It is probably worth mentioning that the Post gets substantial advertising revenue from the drug industry.